Heart failure (HF) represents a significant and growing burden both on patients and the healthcare system:
- It is estimated that more than 1 million people in the UK are living with heart failure.¹
- In England up to 80 per cent of heart failure diagnoses are made in hospital, despite 40 per cent of patients having symptoms that should have triggered an earlier assessment.2
- In the UK, heart failure is responsible for around 2% of the National Health Service (NHS) annual budget and 5% of all emergency hospitalisations.³
These figures highlight the importance of early identification, accurate diagnosis and proactive optimisation of Heart Failure management within primary care, to improve patient outcomes and reduce hospital admissions.
Preventing cardiovascular disease and early diagnosis of heart failure
The Primary Care Networks’ (PCN) Direct Enhanced Services contract asks PCNs to focus on cardiovascular prevention, including the early diagnosis of HF.
When reviewing the local data at Debden Health Group (DHG) there were discrepancies on HF prevalence and coding accuracy identified across practices within the Group – a PCN within Suffolk and North East Essex (SNEE). Although the overall HF prevalence was 0.72% higher than the national average, it was predicted using Public Health England modelled prevalence estimates, that approximately 169 patients across the PCN may have an un-coded heart failure (fig.1).
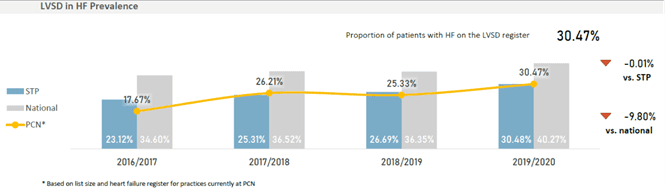
NICE estimates around 50% of HF patients have left ventricular systolic dysfunction (LVSD) or heart failure reduced ejection fraction (HFrEF)4. Identifying these ‘missing’ patients not only helped to improve the Quality Outcomes Framework (QOF) prevalence accuracy but also ensured patients were correctly identified for symptomatic review and monitoring of their condition.
A review of practice processes at DHG found that echocardiogram (echo) coding was inconsistent, along with some inconsistencies in hospital correspondence, which often did not clearly mention a confirmed HF diagnosis. This prevented coders from easily adding patients to the QOF HF register, leading to patients not being coded at the point of diagnosis.
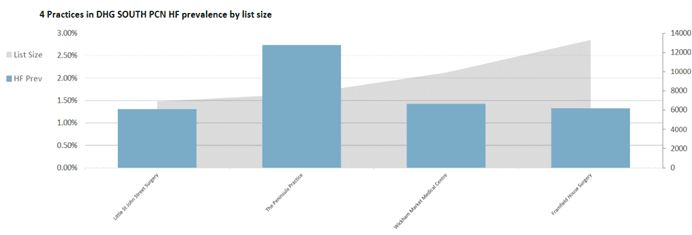
The Peninsula Practice, part of DHG, demonstrated significantly higher HF prevalence compared to other practices, possibly due to the presence of an existing ‘echo coding protocol’ (fig.2).
Implementing this protocol across the PCN became a key part of the project, aiming to standardise how echos and new HF diagnosis were coded. Additionally, it was found that some patients had not been optimised on optimum medication, such as the four pillars of
HF treatment, and these patients may not have always received regular annual reviews of their condition.
DHG proposed a project that would standardise coding practices across the PCN to ensure accurate HF identification, improve QOF performance and enable appropriate clinical management. Through early identification and intervention, the intended outcome of the project was to reduce emergency admissions and associated admission costs for this cohort of patients; whilst also increasing practice QOF income through prevalence adjustments, improving quality of QOF reviews and reducing QOF exception rates.
The project aimed to:
- Ensure all patients with HF receive a comprehensive annual review, including symptom assessment and medication optimisation.
- Titrate therapy appropriately for patients with HF preserved ejection fraction (HFpEF) and HF mildly reduced ejection fraction (HFmrEF).
- Optimise HFrEF patients on the four pillars of medications where clinically appropriate – ARNI/ACE Inhibitor/ARB (Angiotensin Receptor-Neprilysin Inhibitor/Angiotensin Converting Enzyme Inhibitor/Angiotensin Receptor Blocker), Beta-Blockers, Mineralocorticoid Receptor Antagonists (MRAs), and Sodium-glucose cotransporter-2 (SGLT2) Inhibitors.
- Standardise coding and data quality across the PCN by adapting the pre-existing ‘echo coding protocol’ at The Peninsula Practice.
- Enable proactive case finding and management to reduce emergency HF admissions.
The project was developed in three phases:
Phase 1 – Case Finding (2022): Improve coding accuracy and increase HF prevalence by identifying uncoded cases and implementing a revised coding protocol.
Phase 2 – HF Management (2023): Enhance clinical care through staff education, upskilling HF leads, developing an HF protocol and introducing Multidisciplinary Team (MDT) meetings.
Phase 3 – Wider Implementation: Share learning across all PCN practices and potentially extend the model across the wider SNEE region.
The PCN identified a need to improve the accurate coding of HF diagnosis and classification of HFrEF/ LVSD. Through phase one of the project, case finding work and an updated PCN Coding Protocol for incoming hospital correspondence aimed to increase HF prevalence so that patients could be correctly managed and optimised on the four pillars of care.
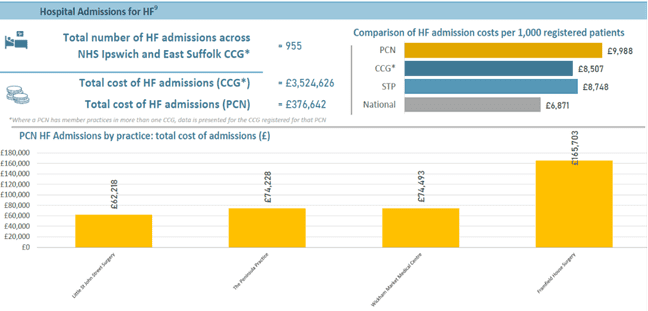
Local Population Health Management data also revealed a high cost associated with HF-related hospital admissions, with many patients presenting with decompensated HF symptoms without a prior HF diagnosis (fig 3).
This highlighted the potential for earlier identification and proactive management within primary care to both reduce avoidable hospital admissions and prolong and improve the quality of life of HF patients.
An implementation guide
Challenges in heart failure management and PCN response
HF reviews have been incentivised through QOF for many years, however in 2020/21 only 31% of HF patients in SNEE received a HF review.
Patients who were not managed by community or hospital HF services may not have received the same standard of reviews as those who were managed by these specialist services. Furthermore, there was variable confidence among clinicians in DHG PCN in recognising HF categories and managing them. Many clinicians were not confident or fully aware of:
- The four pillars of HFrEF management; and
- The differences between HFrEF, HFmrEF, and HFpEF.
The barriers identified
Several system-level and communication barriers may have contributed to variation in management:
- Discharge and outpatient letters from secondary care sometimes lacked clarity regarding the type of HF or guidance on initiating and up-titration to the 4 pillars of treatment.
- Echo results were not consistently shared with primary care, attributing to delays in diagnosis and treatment and may have added to uncertainty over what type of HF a patient had been diagnosed with.
PCN Approach – Bridging the Gap
To address these challenges DHG worked closely with community HF nurses to bridge the gap between primary and secondary care. The PCN nominated an Advanced Nurse Practitioner (ANP) HF Lead who was upskilled to manage HF patients more comprehensively and who, as a result, developed a HF protocol to support DHG clinicians.
Key actions included
- Development of an HF management protocol covering diagnostic pathways, HF category classification and medication management aligned with the four pillars of therapy.
- Delivery of educational MDT sessions to increase clinician confidence in HF diagnosis and management, starting at Framfield House Surgery as a proof of concept, before rolling out across the PCN.
- An HF MDT, involving community HF nurses and PCN clinicians was established, held every 2–3 months, to review and manage complex patients.
Upskilling the Wider PCN Team
The project also focused on upskilling the wider PCN workforce to enable earlier identification and intervention of HF:
- Health Care Assistants (HCAs) and practice nurses were trained and empowered to recognise early HF symptoms during routine appointments or long-term condition reviews and to signpost these patients to the GP. BNP blood tests were introduced to enable and improve earlier HF diagnosis.
- Clinicians were encouraged to use the HF protocol during reviews to ensure consistency and quality across all patients.
The HF Lead ANP acted as the point of contact with the HF MDT, for management of more complex patients. This structured, team-based approach supported earlier detection, consistent management and better alignment with NICE guidance across all practices in the PCN.
Outlining the operational context
NHS England: PCN Direct Enhanced Services – Cardiovascular Disease Prevention Supplementary Guidance
NHS Long Term Plan – CVD: Supporting the early detection of heart failure and heart valve disease through increasing access to diagnostic testing in primary care.
QOF Contract – HF007. The percentage of patients with a diagnosis of heart failure on the register, who have had a review in the preceding 12 months, including an assessment of functional capacity and a review of medication to ensure medicines optimisation at maximal tolerated doses
SNEE Joint Forward Plan – places priority on CVD and aims for 5% reduction in acute admissions with a first presentation of heart failure.
Summary of support offered
- Initial analytical and data support provided by Novartis, included access to Optum data and the Interface Clinical Services CoAM Tool report, to support case finding and coding accuracy work.
- Collaboration with Community Heart Failure Specialist Nurses, providing clinical input, patient reviews and attendance at regular HF MDT meetings every 2–3 months to support shared management of complex cases.
- The work that DHG has done on heart failure has been used as the basis for a role out of the service in the West Ipswich area which will then inform national learning from the national neighbourhood improvement programme pilots (NNIP).
- DHG based much of the protocol and guidance on the European Society of Cardiology (ESC) – 2023 focussed update on heart failure 6.
Impact of the programme
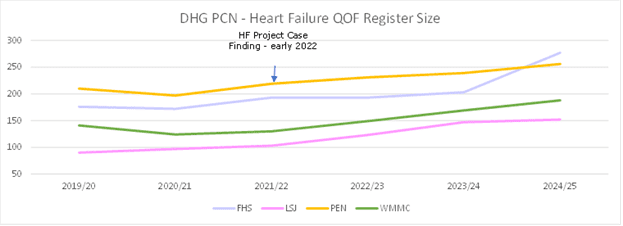
The PCN successfully increased the HF register size through:
- Introducing a unified coding protocol and SystmOne template across the PCN for echocardiograms and cardiology letters, to ensure ejection fraction data is consistently captured and that heart failure is correctly classified (HFpEF, HFmrEF, HFrEF).
- Case finding using Ardens reports: A total of 148 patients were initially reviewed as part of case finding in 2022 – with 37 patients added to the HF register. Patients already on the HF register without an HF classification were also reviewed. 227 patients were subsequently added to the ‘HF2 Register’ (for those with LVSD/reduced ejection fraction).
National QOF prevalence rose from 0.9% when the project stated in 2022, to 1.1% in 2024/25, DHG PCN Practices maintain higher than national average QOF prevalence:
- Framfield at 1.4%
- Little St Johns at 2.1%
- Peninsula Practice at 3.5%
- Wickham Market MC at 1.7%
Standardisation of coding for incoming hospital correspondence across the PCN ensured that all patients with a new diagnosis of HF were promptly added to the QOF HF register and appropriately flagged for review. The coding protocol also ensures all new HF diagnoses are communicated directly to the patient’s GP, so they can communicate the diagnosis to patients and review or optimise medication as required.
In early 2023 the desktop review of Framfield House patients on the HF02 (LVSD/HFrEF) register began to stratify patients based on their latest results and symptoms, whilst avoiding duplication for those already under the community HF nurse review. This led to enhanced reviews by the HF lead ANP of 138 patients on the ‘HF02’ register (19 already under the community HF nurses) to clarify diagosis, check recent BNP/echo results, assess symptoms and optimise medication. The reviews presented an improvement in care for this cohort of patients, as all received an indepth HF review and requests for up to date tests.
Through discussions with patients, the HF Lead ANP also helped to support patients with understanding their diagnosis and prognosis, the benefits of taking specific medications to improve both symptoms and management of their condition. Optimising patients on the four pillars has shown to extend life expectancy, reduce HF related hospital admissions and enhance the quality of life for those with HFrEF 7.
PCN Wide Implementation and Workforce Development
The HF Project was initiated at Framfield House Surgery as a pilot but has since been adopted across all four practices within the Deben Health Group (DHG) PCN.
Through the upskilling of a dedicated HF Lead ANP, the PCN now has an in-house clinical expert in heart failure management who also acts as a liaison with community HF nurses. This collaboration led to the establishment of HF MDT meetings, the first of their kind in the area, enabling stronger integration between primary, community and secondary care services.
Previously, patients required referral to the already overstretched community HF service, sometimes resulting in delays in treatment initiation. With the new model, evidence-based HF therapy can now be confidently initiated in primary care, reducing both the burden on community services and the need for patients to engage with multiple care providers.
This project supported workforce development and empowerment within the PCN:
- The HF Lead ANP expanded their expertise and took on responsibility for long-term condition management.
- A nurse-led HF management protocol was developed, enabling consistent patient HF reviews.
As the project expanded, the HF Lead ANP began completing reviews across all four PCN practices, supporting QOF achievement and alleviating GP workload by shifting elements of chronic disease management to ANP’s. This cross-practice approach also highlighted variation in clinician confidence and training, identifying opportunities for targeted education — particularly around the four pillars of HFrEF management.
By optimising treatment earlier and achieving better symptom control, the expectation is that previously high-demand HF patients will require fewer clinical appointments and hospital visits, leading to improved patient outcomes and a more sustainable workload across the PCN.
Impact and Evaluation
However, the project has already demonstrated some measurable financial and quality benefits at practice level:
- QOF income has increased due to adjustments in prevalence and the expansion of the HF register.
- The Heart Failure QOF domain, valued at 29 points, has contributed significantly to this improvement.
- The value of individual QOF points has increased during this period.
- 2021/22 CQRS reports indicated an unusual peak (41 points) in income for HF003/ HF006 compared with other years (fig.4)
These findings may demonstrate that, while the broader system impact will require a longer period of evaluation, the project has already delivered benefits for practices in terms of data quality, register accuracy and QOF performance.
An implementation guide
DHG Early identification and optimisation of heart failure
Step 1: Retrospective case finding.
Step 2: Ongoing early identification.
Step 3: Identifying and diagnosis.
Step 4: The heart failurereview review.
Click the link above to learn more
Figures and charts
Figures and charts
Figure 1: QOF Heart Failure Prevalence Data: NHS England – NHS Digital. (2025). Quality and Outcomes framework – Official Statistics. [Online]. digital.nhs.uk. Last Updated: 28 August 2025. Available at: https://digital.nhs.uk/data-and-information/publications/statistical/quality-and-outcomes-framework- [Accessed 10 March 2026].
Figure 2: QOF Heart Failure Prevalence Data: NHS England – NHS Digital. (2025). Quality and Outcomes framework – Official Statistics. [Online]. digital.nhs.uk. Last Updated: 28 August 2025. Available at: https://digital.nhs.uk/data-and-information/publications/statistical/quality-and-outcomes-framework- [Accessed 10 March 2026].
Figure 3: Heart failure admissions (England) HES inpatient data April 2019-March, 2020. Novartis data on file.
Figure 4: QOF database. (2024). NHS England Heart Failure. [Online]. gpcontract.co.uk. Available at: https://www.gpcontract.co.uk/browse/ENG/Heart%20Failure/24 [Accessed 10 March 2026].
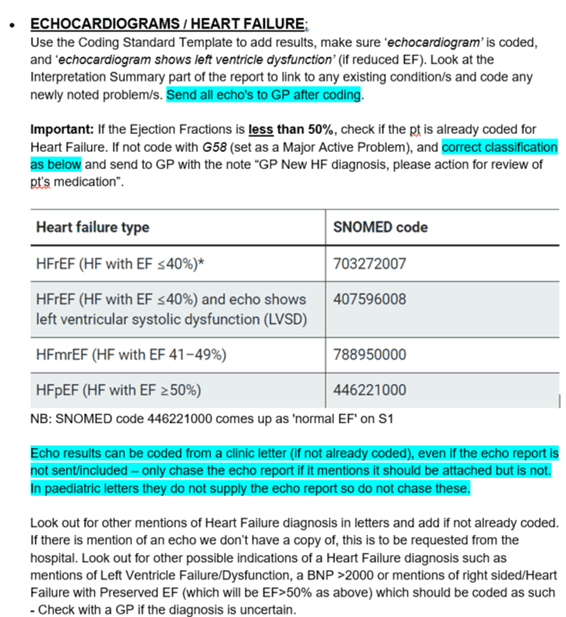
Figure 5: Coding protocol example.
Figure 6: Figure 4: QOF database. (2024). NHS England Heart Failure. [Online]. gpcontract.co.uk. Available at: https://www.gpcontract.co.uk/browse/ENG/Heart%20Failure/24 [Accessed 10 March 2026].
References
References
- British Heart Foundation. (2026). Facts and Figures. [Online]. but.org.uk. Last Updated: 2026. Available at: https://www.bhf.org.uk/what-we-do/news-from-the-bhf/contact-the-press-office/facts-and-figures [Accessed 10 March 2026].
- British Heart Foundation. (2026). England Cardiovascular Disease Factsheet. [Online]. bhf.org.uk. Available at: www.bhf.org.uk/-/media/files/for-professionals/research/heart-statistics/bhf-cvd-statistics-england- [Accessed 10 March 2026].
- Fletcher, Robert, A. et al. (2025). Contemporary epidemiology of hospitalised heart failure with reduced versus preserved ejection fraction in England: a re. The Lancet Public Health. 9(11), pp.e871.
- National Institute for Health and Care Excellence. (https://cks.nice.org). How common is it?. [Online]. cks.nice.org. Last Updated: September 2025. Available at: https://cks.nice.org.uk/topics/heart-failure-chronic/background-information/prevalence/#:~:text=Prev [Accessed 10 March 2026].
- British Heart Foundation. (2015). An integrated approach to managing heart failure in the community. [Online]. [Accessed 2nd October 2020]. Available from: https://www.bhf.org.uk/informationsupport/publications/healthcare-and-innovations/an-integrated-approach-to-managing-heart-failure-in-the-community . National Institute for Cardiovascular Outcomes Research (NICOR). (2019). National Heart Failure Audit 2019 Summary Report (2017/18 [Accessed 2nd October 2020]. Available from: https://www.nicor.org.uk/wp-content/uploads/2019/09/Heart-Failure-2019-Report-final.pdf.
- European Society of Cardiology. (2023). 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. [Online]. escardio.org. Last Updated: 25 August 2023. Available at: https://www.escardio.org/guidelines/clinical-practice-guidelines/all-esc-practice-guidelines/focused [Accessed 10 March 2026].
- Tromp, J, MD. et al. (2022). A Systematic Review and Network Meta-Analysis of Pharmacological Treatment of Heart Failure With Reduced Ejection Fracti. JACC: Heart Failure. 10(2), pp.73-84. [Online]. Available at: https://doi.org/10.1016/j.jchf.2021.09.004. [Accessed 10 March 2026].
Share your idea
Do you have a great idea that could deliver meaningful change in the real world?
Get involved